

INTRODUCTION
The need for factor concentrate (FC) prior to uncomplicated endoscopies in persons with hemophilia (PWH) is not well characterized. Infusion of FC is time consuming, costly, and increases risk of inhibitor development. There is no general consensus on management of PWH undergoing endoscopies and the incidence of bleeding is not well established.
At our Hemophilia Treatment Center (HTC), our standard of care (SOC) for many years was to manage PWH with an infusion of FC prior to any endoscopy for any indication regardless of severity of hemophilia. In November 2017, we changed our SOC for persons with mild hemophilia (factor VIII or IX >5%) to use only antifibrinolytics pre-endoscopy for those in whom no procedural intervention was anticipated, followed by infusion of FC post-endoscopy if a biopsy or polypectomy was performed or if there was bleeding associated with the procedure. Persons with moderate or severe hemophilia (factor VIII or IX ≤5%) continued to receive infusion of FC prior to all endoscopies.
We report our experience managing PWH of all severities undergoing EGD and colonoscopy between 2008 and 2019. We compare incidence of bleeding, cost of medical care, and outcomes before and after the change in SOC for persons with mild hemophilia.
METHODS
Subjects were identified from a database of patients treated at our HTC. Those with factor VIII inhibitors were excluded. Cost of FC and antifibrinolytics were determined from average wholesale pharmacy prices in 2019. Gastrointestinal (GI) bleeding was assessed by review of medical records within 30 days after endoscopy. Documentation of any patient or clinician reported hematemesis or rectal bleeding, requiring or not requiring medical attention or treatment, was recorded as GI bleeding. Adequacy of hemostasis, as assessed by review of medical records, was classified as poor if the subject had unexpected hypotension, required intensive or intermediate care, or transfusion; fair if unplanned doses of FC were required, but the event did not meet criteria for poor hemostasis; and excellent for events that did not meet any of the above criteria.
RESULTS
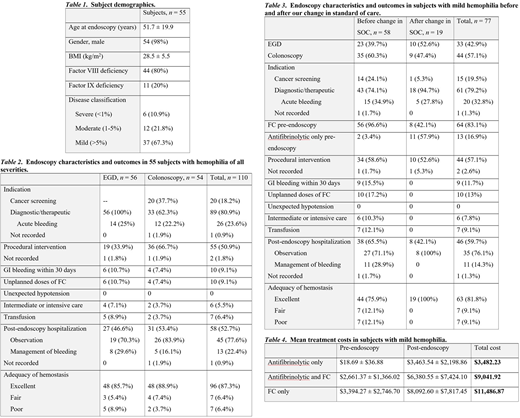
Sixty-seven subjects met eligibility criteria; 12 were excluded due to inadequate records of endoscopies. Data were collected on 110 endoscopies performed in 55 subjects, range 1 to 5 per subject. Subject demographics are noted in Table 1. Endoscopy characteristics and outcomes are shown in Table 2.
GI bleeding occurred within 30 days after 10 endoscopies prior to the change in SOC. This included 7 endoscopies performed because of preexisting bleeding due to esophageal varices, or gastric, duodenal, or colonic ulcers. In addition, post endoscopy bleeding occurred in one patient after colonoscopy following the use of hot snare cautery resection of polyps, and in another after resection of a rectal polyp by cold snare following an EGD with colonoscopy. No GI bleeding occurred within 30 days of the endoscopies performed after we changed our SOC. FC was used prior to 97.1% of 68 endoscopies performed before we changed our SOC, compared to 73.8% of 42 endoscopies performed after. Hospital stay of 2 days was equivalent across all groups when subjects with preexisting bleeding were excluded. Hemostasis was excellent in 79.4% of endoscopies before we changed our SOC and 100% of endoscopies after.
Endoscopy characteristics and outcomes in subjects with mild hemophilia before and after we changed our SOC are shown in Table 3. Reasons for using FC pre-endoscopy in these subjects included preexisting bleeding, planned intervention, or anticipated complex procedure.
Treatment costs in subjects with mild hemophilia are noted in Table 4.
CONCLUSION
We describe our HTC's experience with endoscopies in PWH. In our cohort of persons with mild hemophilia, we demonstrate that the use of antifibrinolytics rather than FC pre-endoscopy did not result in any difference in adequacy of hemostasis or development of GI bleeding within 30 days post endoscopy. This practice was associated with significant cost-savings and no difference of hospitalization rate or length of stay.
We conclude that persons with mild hemophilia, who are not actively bleeding or undergoing complex procedures, can be safely managed with antifibrinolytics alone pre-endoscopy. However, patient-specific and procedure-specific factors must be considered when determining the appropriate pre-endoscopy treatment for bleeding prophylaxis in PWH.
Eyster:Novo Nordisk: Research Funding; SPARK: Research Funding; Sanofi: Research Funding; Baxalta/Shire: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal